
PCOS Treatment Eligibility Checker
This tool helps determine if Desogestrel-Ethinyl Estradiol is generally suitable based on key medical criteria from PCOS treatment guidelines.
Please complete the form to check eligibility.
Imagine battling irregular periods, unwanted facial hair, and stubborn weight gain while your doctor keeps pointing to the same hormonal imbalance. For many women with Polycystic Ovary Syndrome is a complex endocrine disorder that triggers insulin resistance, androgen excess, and anovulation. One drug combination often pops up in the conversation: Desogestrel‑Ethinyl Estradiol is a combined oral contraceptive (COC) that blends the progestin desogestrel with the estrogen ethinyl estradiol. Below we unpack why that combo matters, who benefits most, and how it stacks up against other PCOS options.
Key Takeaways
- Desogestrel‑EE regulates menstrual cycles and lowers androgen levels in most women with PCOS.
- Its low‑androgenic progestin reduces the risk of acne and hirsutism compared with older COCs.
- When insulin resistance is the main driver, adding metformin often improves outcomes.
- Contraindications include smoking over age 35, uncontrolled hypertension, and active liver disease.
- Regular follow‑up every 3-6 months helps catch side effects early and fine‑tune therapy.
How Desogestrel‑Ethinyl Estradiol Works in PCOS
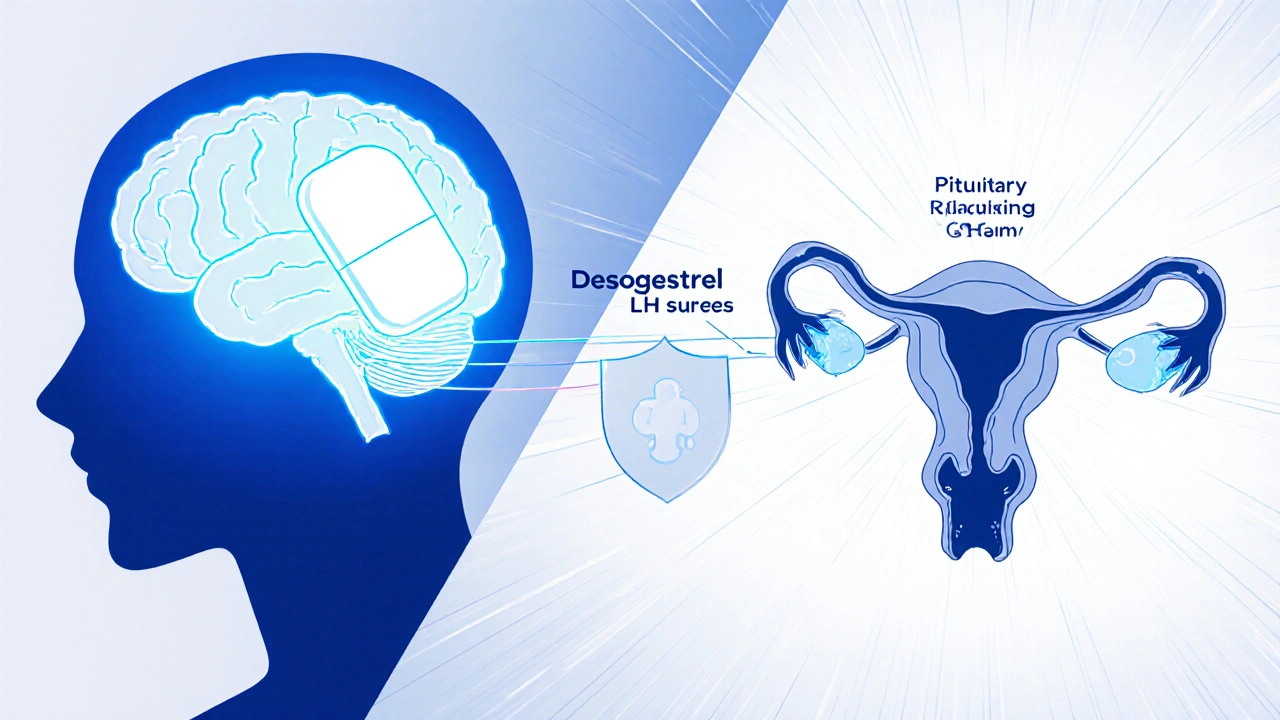
At its core, a COC suppresses the hypothalamic‑pituitary‑ovarian (HPO) axis. The estrogen component, ethinyl estradiol, tricks the brain into thinking estrogen levels are sufficient, which in turn lowers follicle‑stimulating hormone (FSH) spikes. Desogestrel, a third‑generation progestin, blocks luteinizing hormone (LH) surges that would otherwise stimulate the ovaries to produce excess androgens.
This double‑hit does three things that matter for PCOS:
- Cycle regularity: By stabilizing the HPO axis, bleeding becomes predictable, making it easier to track ovulation windows.
- Androgen suppression: Desogestrel has a weak androgenic profile, so it doesn’t add to existing testosterone levels. In many studies, women on desogestrel‑EE saw a 30‑40% drop in free testosterone.
- Protection against endometrial hyperplasia: Continuous estrogen exposure without progestin can thicken the uterine lining; desogestrel prevents that risk.
Because the pill also raises sex‑hormone‑binding globulin (SHBG), more circulating testosterone gets bound, further lowering the amount that can act on skin and hair follicles.
Benefits Beyond Hormone Balance
While the primary goal is to control hormones, women often notice secondary improvements:
- Reduced acne and facial hair: Lower free testosterone means fewer oily sebaceous glands and slower hair growth in androgen‑sensitive areas.
- Improved lipid profile: Ethinyl estradiol modestly raises HDL (good cholesterol) and can lower LDL when used at low doses.
- Potential weight stabilization: Some patients report less binge‑eating cravings, likely tied to steadier insulin swings.
It’s worth noting that the pill does not directly treat insulin resistance. If a woman’s glucose levels remain high, clinicians usually add Metformin - an insulin‑sensitizing biguanide that lowers hepatic glucose output and improves peripheral uptake.
How It Compares with Other PCOS Therapies
Choosing the right regimen is a balancing act between symptom control, side‑effect profile, and long‑term health goals. The table below contrasts desogestrel‑EE with three common alternatives.
| Option | Primary Action | Androgen Effect | Insulin Impact | Typical Use Cases |
|---|---|---|---|---|
| Desogestrel‑Ethinyl Estradiol (COC) | HPO axis suppression | Low‑androgenic | Neutral | Irregular cycles, acne, hirsutism |
| Drospirenone‑Ethinyl Estradiol (COC) | HPO axis suppression | Anti‑androgenic | May improve insulin sensitivity | Severe acne, water retention concerns |
| Cyproterone Acetate‑Ethinyl Estradiol (COC) | HPO axis suppression + strong anti‑androgen | Strong anti‑androgenic | Neutral | Pronounced hirsutism, severe seborrhea |
| Metformin (oral) | Improves insulin sensitivity | Indirect (lowers insulin‑driven androgen production) | Improves | Predominant insulin resistance, BMI >30 |
| Spironolactone (anti‑androgen) | Blocks androgen receptors | High anti‑androgenic | Neutral | Persistent acne/hirsutism despite COC |
Notice that desogestrel‑EE sits in the sweet spot: it controls cycles, modestly lowers androgens, and avoids the potassium‑sparing effect of spironolactone, which can be a concern for women with hypertension.
Who Is the Best Candidate?
Ideal patients share a few common traits:
- Age 18‑35, with no smoking habit (or less than 10 cigarettes/day).
- Predominant symptoms of menstrual irregularity, acne, or mild hirsutism.
- Normal blood pressure and no personal history of thromboembolism.
- Desire for contraception (the pill doubles as birth control).
If a woman presents with significant obesity (BMI >35) and marked insulin resistance, a clinician might start with metformin first, then layer desogestrel‑EE once glucose control improves.
Contraindications-often summarized as "CHC contraindications"-include active liver disease, uncontrolled hypertension, a history of stroke, or migraine with aura. In those cases, non‑hormonal options such as Lifestyle modification (diet, exercise, weight loss) become the frontline strategy.
Practical Prescription Guide
Typical dosing follows a 21‑day active pill regimen followed by a 7‑day hormone‑free interval. Each active tablet contains 150 µg desogestrel and 30 µg ethinyl estradiol. Here’s a step‑by‑step plan most providers use:
- Baseline labs: fasting glucose, lipid panel, liver enzymes, and blood pressure.
- Discuss contraception goals and potential side effects (nausea, breast tenderness, spot bleeding).
- Start the pill on day 1 of the menstrual cycle or on a random day with a 7‑day backup method.
- Schedule follow‑up at 3 months to review symptom change, weight, and any adverse events.
- If acne/hirsutism persists, consider adding Spironolactone at 50‑100 mg daily.
Common side effects are mild and often fade after the first cycle. Rare but serious concerns include deep‑vein thrombosis; patients should be educated to seek immediate care for leg pain or sudden shortness of breath.
Frequently Asked Questions
Can Desogestrel‑EE help me get pregnant?
The pill prevents ovulation, so it’s not a fertility aid. However, after stopping, most women resume ovulation within one to two cycles, making it a reversible option for those who plan pregnancy later.
Is the pill safe if I have mild hypertension?
Mild, well‑controlled hypertension is not an absolute contraindication, but clinicians often prefer a non‑estrogenic method or closely monitor blood pressure every month.
Do I need to take the pill continuously?
Standard COCs follow a 21‑day active/7‑day placebo schedule, which mimics a natural menstrual bleed. Extended‑cycle regimens (84‑day active) are an option if you want fewer periods, but discuss with your doctor first.
Can I combine the pill with metformin?
Yes. Metformin addresses insulin resistance while the COC manages hormone‑driven symptoms. The combination is common and well‑tolerated.
What should I watch for as a warning sign?
Sudden leg swelling, chest pain, severe headache, or vision changes could signal a blood clot. Seek emergency care if any appear.
By understanding how desogestrel‑ethinyl estradiol fits into the broader PCOS toolbox, you can work with your provider to craft a plan that tackles irregular cycles, skin concerns, and long‑term metabolic health-all while keeping contraception simple.



Andrew Hernandez
October 20, 2025 AT 14:20Desogestrel‑EE is a solid option for many with PCOS.
Kate McKay
October 23, 2025 AT 16:20It’s great when a treatment hits several problems at once.
While the pill won’t cure insulin resistance, it can smooth out cycles and clear up skin.
Most women notice lighter periods within a couple of months, which makes tracking easier.
The reduction in free testosterone often means fewer break‑outs and less stubborn facial hair.
I’ve seen patients who were skeptical at first become believers after the first quarter.
Pairing the COC with a low‑dose metformin can tackle the metabolic side while keeping hormone levels in check.
Keep an eye on blood pressure; the estrogen component can raise it slightly in some folks.
If you’re a non‑smoker under 35, the clot risk stays low, especially with desogestrel’s favorable profile.
Lifestyle changes still matter – regular exercise and a balanced diet amplify the benefits.
Don’t forget to schedule a follow‑up at three months; that’s when you can fine‑tune dosage or add an anti‑androgen if acne persists.
Some women experience mild nausea at the start, but it usually fades after the first cycle.
Weight changes are modest, but many report reduced cravings, which helps with weight control.
If you have a history of migraines with aura, discuss alternatives with your doctor.
The pill also protects the endometrium, reducing the long‑term risk of hyperplasia.
Overall, it’s a versatile tool in the PCOS toolbox.
Stick with it for at least six months before judging effectiveness.
Demetri Huyler
October 26, 2025 AT 17:20American endocrinology guidelines have long championed third‑generation progestins for their lower androgenic footprint. Desogestrel‑EE exemplifies that approach, marrying efficacy with a safety profile that holds up under rigorous FDA scrutiny. It’s a pragmatic choice that aligns with our nation's standards of care.
JessicaAnn Sutton
October 29, 2025 AT 19:20While clinical data support the recommendation, it remains essential to contextualize therapy within each patient’s ethical framework, ensuring that choices are not merely driven by regulatory endorsement but by holistic well‑being.
Israel Emory
November 1, 2025 AT 21:20Desogestrel‑EE, when prescribed responsibly, offers a balanced regimen-period regularity, acne mitigation, and contraceptive reliability; however, physicians must vigilantly monitor for hypertension, thrombotic signs, and liver function, especially in patients with pre‑existing risk factors.
Wesley Humble
November 4, 2025 AT 23:20From a pharmacological standpoint, the combination functions via hypothalamic negative feedback, thereby attenuating LH surges and subsequently reducing ovarian androgen synthesis. 📊 Consequently, the net clinical effect aligns with the therapeutic objectives outlined in the source material, rendering the regimen both efficacious and safe when adherence is maintained.
barnabas jacob
November 8, 2025 AT 01:20Yo, the desogestrel‑EE stack is like a bio‑modul8r for the HPO axis, low‑androgenic vibes keep the sebaceous glands chill, but yo watch da liver enzymes – don’t wanna go off the rails.
Vijaypal Yadav
November 11, 2025 AT 03:20In addition to the hormonal mechanisms described, the increased SHBG levels consequent to ethinyl estradiol administration contribute to a reduction in free androgen index, which is a quantifiable marker in PCOS management.
Ron Lanham
November 14, 2025 AT 05:20It is a moral imperative for clinicians to convey the full spectrum of risks associated with any hormonal therapy.
Patients deserve transparent discussion about thrombosis, especially when lifestyle factors such as smoking intersect with pharmacology.
The convenience of a combined oral contraceptive should never eclipse the duty to individualize care.
When a young woman presents with hirsutism, the temptation to prescribe the quickest fix is strong, yet a nuanced assessment yields better outcomes.
The interplay between insulin resistance and androgen excess underscores the necessity of multimodal treatment.
Metformin, though not a panacea, can synergize with desogestrel‑EE to address hyperinsulinemia.
Moreover, the psychosocial impact of acne and unwanted hair cannot be dismissed as merely cosmetic.
It influences self‑esteem, professional confidence, and social interactions.
Therefore, any therapeutic plan must incorporate both physiological and psychological dimensions.
Regular follow‑up appointments serve as checkpoints to reassess efficacy and safety.
Should adverse events arise, prompt alteration of the regimen reflects ethical stewardship.
In sum, the prescriber’s responsibility extends beyond the prescription pad to the holistic well‑being of the patient.
Deja Scott
November 17, 2025 AT 07:20Desogestrel‑EE fits well within a culturally sensitive approach to PCOS management, respecting individual preferences while providing reliable contraception.
Natalie Morgan
November 20, 2025 AT 09:20Embrace the regimen, track your cycles, and celebrate each improvement-consistency fuels confidence.
Mahesh Upadhyay
November 23, 2025 AT 11:20In the grand drama of hormonal imbalance, desogestrel‑EE plays the understated hero, subtly restoring order without stealing the spotlight.
Rajesh Myadam
November 26, 2025 AT 13:20I hear the concerns many share about side effects; remember that open dialogue with your provider can tailor the plan to your comfort and health goals.